Provider Ranking System™ Brings Transparency to Healthcare Cost Dilemma
By Tom Denniston, Account Executive, Denniston Data Inc.
9/2/21
Did you happen to see the recent article from the New York Times titled, “Hospitals and Insurers Didn’t Want You to See These Prices. Here’s Why?” The August 2021, article is about how now a complete list of prices negotiated with private insurers, from every hospital, has been ordered from the federal government to be published. While this has been called unconstitutional by their trade association, and four hospital associations together sued the government to block it, a couple of times, they’ve lost both times. To quote the NYTs article, “This secrecy has allowed hospitals to tell patients that they are getting ‘steep’ discounts, while still charging them many times what a public program like Medicare is willing to pay. And it has left insurers with little incentive to negotiate well.”[1]
None of us used to know the prices before receiving a bill after services were rendered. Even worse, “some insurance companies have refused to provide the information when asked by patients and the employers that hired the companies to provide coverage.”[2] It is sometimes even cheaper to see a provider while having no (or pretending to have no) insurance than when using insurance. To make matters worse, over 20% of overall medical care is unnecessary or harmful according to multiple studies in PubMed.[3]
The article continues, “At multiple hospitals, major health plans pay more than four times the Medicare rate for a routine colonoscopy. And for an M.R.I. scan, some are paying more than 10 times what the federal government is willing to pay.”[4] Employers are the largest purchasers of health insurance and would benefit the most from lower prices. However, most select plans without knowing what they and their workers will pay. But wait, with this new government rule the prices will be published, right? Not necessarily. Many hospitals are now just ignoring this requirement and posting nothing, not to mention seeing no pricing per individual provider.
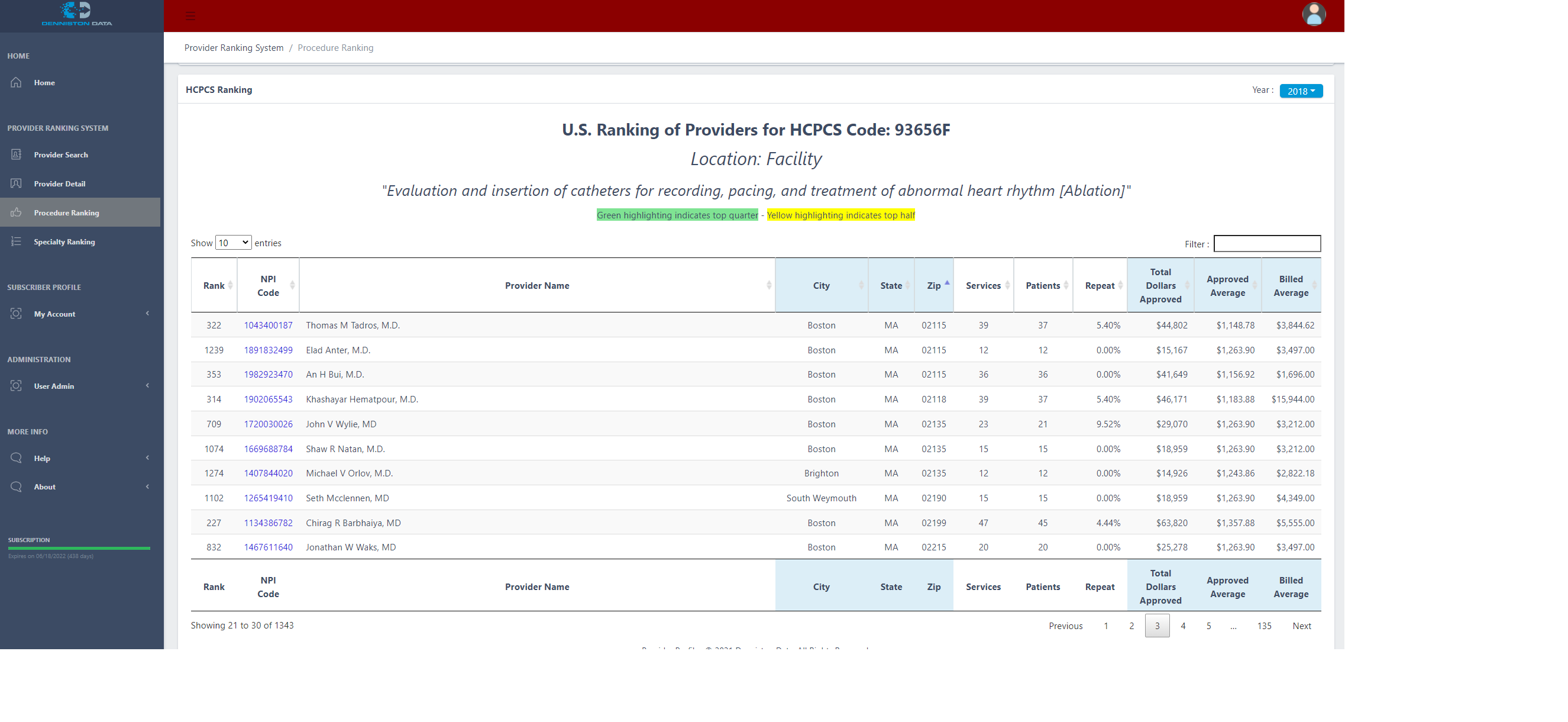
Well, fortunately this recent transparency mandated by the federal government has been put into a user-friendly tool known as the Provider Ranking System (PRS), which provides actual experience data on every provider in the U.S. Over one million providers are covered, including medical doctors and all other types of providers that bill for medical procedures. PRS publishes each provider’s average billed price charged, by year, for every procedure they perform. Searching can be done by either provider or by medical procedure. On top of that, the PRS does not accept advertising or payment to enhance one’s own listing.
PRS also contains the price Medicare allows. As well as what the provider’s average billing rate by procedure is of Medicare’s allowable costs. This enables the user to not only compare providers by their experience in performing a procedure, but by the list prices they charge for each procedure, all based on actual reported data. These can be sorted by the prices a provider charges for the same procedure. Seeing both the list prices and also the approved amount, which PRS has, can be especially helpful when it comes to negotiations.
Any provider can be looked up by their 10-digit NPI (National Provider Identifier) number, or by any combination of last name, first name, city, state, and medical specialty. So now employers don’t need to remain in the dark on budgeting for these healthcare expenses, and neither do consumers.
How about a demo? I’m happy to instruct one myself remotely, or if you’d prefer, here’s our YouTube page for a video, https://www.youtube.com/channel/UCwNFVQ4BN3WMU3zVc8O-dfQ.
[1] Kliff, Sarah and Katz, Josh. Produced by Taylor, Rumsey. “Hospitals and Insurers Didn’t Want You to See These Prices. Here’s Why.” nytimes.com, New York Times, The Upshot, 22 Aug 2021,
https://www.nytimes.com/interactive/2021/08/22/upshot/hospital-prices.html
[2] Kliff, Katz, Hospitals and Insurers
[3] Banks A, Samuel S, Johnson D, Hecker K, McLaughlin K, Reducing physician voiding cystourethrogram ordering in children with first febrile urinary tract infection: evaluation of a purposefully sequenced educational intervention. Can Med Educ J. 2018 Nov; 9(4): e6–e14. Published online 2018 Nov 12, PMID: 30498539, PMCID: PMC626051
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6260512/
[4] Kliff, Katz, Hospitals and Insurers